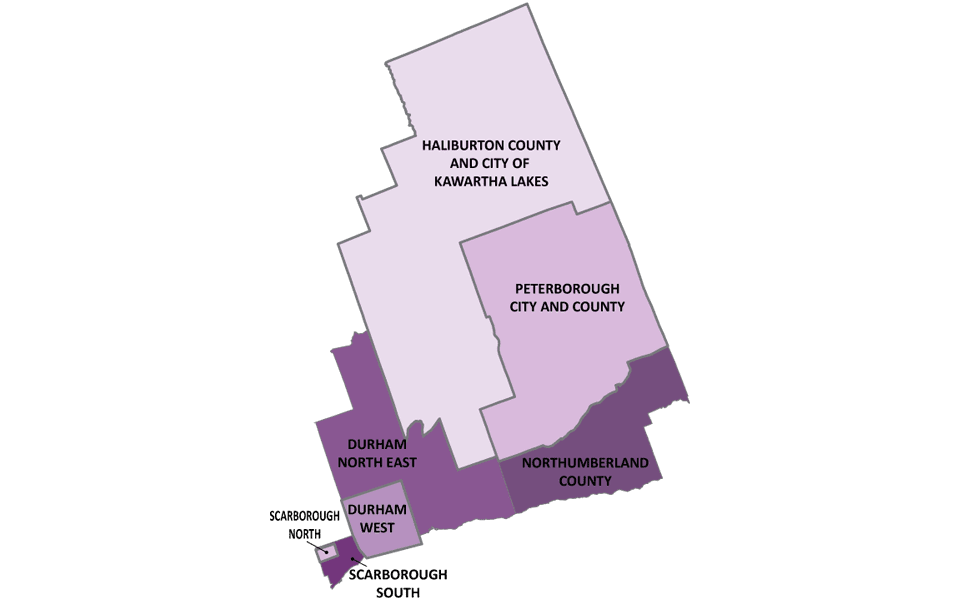
Central East area
We are now Ontario Health atHome (opens in a new tab) , a single organization coordinating local home and community care, long-term care placement and help finding services in the community. Our name has changed but our services remain the same. Patients continue to work with the same patient care teams and can contact us the same way.
Information and Referral
310-2222
Toll-free:1-800-263-3877
Fax1-855-352-2555
TTY:711
Visit Central East Healthline
Central East Area Office Locations
-
Whitby
920 Champlain Court
Whitby, ON, L1N 6K9
-
Scarborough
100 Consilium Place
Suite 801
Scarborough, ON, M1H 3E3
-
Port Hope
151A Rose Glen Road
Port Hope, ON, L1A 3V6
-
Lindsay
370 Kent Street West
Unit 11
Lindsay, ON, K9V 6G8
-
Campbellford
119 Isabella Street
Unit 7
Campbellford, ON, K0L 1L0
-
Peterborough
700 Clonsilla Avenue
Suite 202
Peterborough , ON, K9J 5Y3
-
Haliburton
73 Victoria Street
P.O. Box 793
Haliburton, ON, K0M 1S0
Compliments and Concerns?
Please share your feedback with your care coordinator. You may also share compliments or concerns in the following ways:
Email: CE.patientrelations@ontariohealthathome.ca
Phone: 1-800-263-3877 ext. 2273
Mail: Ontario Health atHome
Compliments and Concerns
Whitby Branch
920 Champlain Court
Whitby, ON L1N 6K9
Newsroom and Media Relations
Visit our newsroom for more information on news and events.
For all media-related enquiries, please contact media@ontariohealthathome.ca.
For non-media-related enquiries, please visit the Contact Us page to access additional contact information.
Accessibility Documents
Publications
- Behavioural Specialized Units Info Sheet
- Behavioural Specialized Units Quick Guide
- Centralized Diabetes Intake Fact Sheet
- Community Nursing Clinics
- Connecting You with Care
- Community Palliative Care Nurse Practitioner Program Fact Sheet
- Family-Managed Home Care Program
- Guide to Placement in Long-Term Care Homes
- High Intensity Supports at Home (HISH) Program
- Mental Health and Addictions Nurses in School (MHAN) Fact Sheet
- Mental Health and Addictions Nurses in Schools – Patient Flyer
- Patient Welcome Booklet
- Rapid Response Nurses Fact Sheet
- Telehomecare Fact Sheet for Doctors
- Wound Care Program
Forms
| Title | Summary | Tags | Categories | Last modified date | Link | hf:doc_tags | hf:doc_categories | hf:file_type |
|---|---|---|---|---|---|---|---|---|
| Request For Assessment Form | Phone: 800-263-3877 | Central East | Forms | September 11, 2025 | central-east | forms | ||
| LTC Health Assessment – Ontario Health atHome | This form is to be used for completion of the assessment required under the Fixing Long-Term Care Act, 2021 when a person applies for a determination of eligibility for long-term care home admission. The required assessment is of the applicant’s physical and mental health, and the applicant’s requirements for medical treatment and health care. This assessment must be made by a physician or registered nurse. | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | Forms | September 10, 2025 | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | ||
| Symptom Response Kit (SRK) for End-of-Life Order Form | Timing and placement of the Symptom Response Kit (SRK) requires careful consideration (i.e. prognosis is less than six months; patient expected to deteriorate quickly) with goal of avoiding emergency room visit or hospital admission. | Central East, Champlain, South East | Forms | August 7, 2025 | central-east champlain south-east | forms | ||
| Negative Pressure Wound Therapy Referral Form | Note: NPWT will continue to be assessed in the community, and settings may be reviewed based on exudate and patient tolerance. Continuation of NPWT is dependent on wound healing goals being met. Maximum treatment time for NPWT is 8 weeks. | Central East | Forms, Medical Equipment and Supplies | May 30, 2025 | central-east | forms medical-equipment-and-supplies | ||
| Demande de détermination de l’admissibilité à l’admission à un foyer de soins de longue durée | Veuillez suivre ces instructions (S’ouvre dans un nouvel onglet) Formulaire fourni par le ministère des Soins de longue durée en vertu de la Loi de 2021 sur le redressement des soins de longue durée. Si vous souhaitez être admis dans un foyer de soins de longue durée (SLD), vous devez remplir ce formulaire. Ces renseignements sont requis par Santé à domicile Ontario, le coordonnateur du placement désigné pour les foyers de SLD, afin de déterminer si vous êtes admissible à l’admission. Santé à domicile Ontario peut recueillir d’autres renseignements personnels sur la santé auprès de vos fournisseurs de soins de santé afin de déterminer votre admissibilité. Santé à domicile Ontario peut également utiliser et divulguer les renseignements aux mêmes fins. | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | Forms | May 1, 2025 | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | ||
| Application for Determination of Eligibility for LTC | Important Note: Please follow these instructions (opens in a new tab) to access the form. Form provided by the Ministry of Long-Term Care under the Fixing Long-Term Care Act, 2021. If you wish to be admitted to a long-term care (LTC) home, you must fill out this form. This information is required by Ontario Health atHome, the designated placement co-ordinator for LTC homes, to determine if you are eligible for admission. Ontario Health atHome may collect additional personal health information from your health care providers | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central | Forms | May 1, 2025 | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central | forms | ||
| Formulaire de demande pour la divulgation de renseignements personnels | Formulaire de demande pour la divulgation de renseignements personnels. En vertu de la Loi de 2004 sur la protection des renseignements personnels sur la santé Veuillez | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | Forms | September 19, 2024 | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | ||
| Request for Release of Personal Health Information | Request for Release of Personal Health Information under the Personal Health Information Protection Act, 2004 | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | Forms | September 19, 2024 | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | ||
| Centralized Diabetes Intake Referral Form | Centralized Diabetes Intake Referral FormFor Access to Diabetes Education Programs and the Centre for Complex Diabetes Care Phone: 1-888-997-9996 Fax: 1-905-444-2544 Toll Free Fax: 1-844-731-2161 | Central East | Forms | July 25, 2024 | central-east | forms | ||
| Feedback Form – How did we do today? | At Ontario Health atHome, we are committed to leading the advancement of an integrated sustainable health care system that ensures better health, better care and better value. Your feedback is important to us. | Central East | Forms | July 10, 2024 | central-east | forms | ||
| Mental Health and Addictions Nurse (MHAN) Referral Form | To be eligible to receive Ontario Health atHome MHAN services the student must be: | Central East | Forms | July 3, 2024 | central-east | forms | ||
| COPD and Heart Failure Telehomecare Referral Form – FR | Formulaire de renvoi à Télésoins à domicile pour les patients atteints d’une maladie pulmonaire obstructive chronique (MPOC) ou d’une insuffisance cardiaque | Central East | Forms | June 28, 2024 | central-east | forms | ||
| Formulaire de renvoi à Télésoins à domicile MPOC & d’une insuffisance cardiaque | Centre-Est, Formulaire de renvoi à Télésoins à domicile pour les patients atteints d’une maladie pulmonaire obstructive chronique (MPOC) ou d’une insuffisance cardiaque congestive. | Central East | Forms | January 12, 2024 | central-east | forms | ||
| COPD and Heart Failure Telehomecare Referral Form | Central East – COPD and Heart Failure Telehomecare Referral Form | Central East | Forms | January 12, 2024 | central-east | forms | ||
| PrVEKLURY® Remdesivir Infusion Referral Form | Central East, PrVEKLURY® Remdesivir Infusion Referral Form. Please ensure form is completed for accuracy. | Central East | Forms | December 13, 2023 | central-east | forms | ||
| COVID-19 formulaire de renvoi vers le programme de surveillance | Les patients inscrits au programme de surveillance à distance utilisent une application sur leur téléphone intelligent pour communiquer leurs symptômes à l’infirmière. | Central East | Forms | December 4, 2023 | central-east | forms | ||
| COVID-19 Remote Monitoring Program Referral Form | Patients enrolled in the COVID-19 Remote Monitoring Program use an app on their smartphone to report their symptoms to their nurse. | Central East | Forms | December 4, 2023 | central-east | forms | ||
| MAID Prescription Order Form | Central East Medical Assistance in Dying Prescription Order Form | Central East | Forms | July 25, 2023 | central-east | forms | ||
| Hip and Knee Referral Form | Hip and Knee Referral Form | Central East | Forms | March 31, 2023 | central-east | forms | ||
| Patient Appeal Form | Patient Appeal Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Narcotic Infusion Therapy Referral Form | Narcotic Infusion Therapy Referral Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Infusion Therapy Referral Form | Infusion Therapy Referral Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Hospital Request for Assessment Form | Hospital Request for Assessment Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Hospital Narcotic Infusion Therapy Referral Form | Hospital Narcotic Infusion Therapy Referral Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Hospital Infusion Therapy Referral Form | Hospital Infusion Therapy Referral Form | Central East | Forms | September 19, 2022 | central-east | forms | ||
| Community Paramedicine Referral Form | Community Paramedicine Referral Form | Central East | Forms | September 19, 2022 | central-east | forms |