South West area
We are now Ontario Health atHome (opens in a new tab) , a single organization coordinating local home and community care, long-term care placement and help finding services in the community. Our name has changed but our services remain the same. Patients continue to work with the same patient care teams and can contact us the same way.
Information and Referral
310-2222
Toll-free:1-800-811-5146
Fax:519-472-4045
TTY:711
Email:SWAccessIandR@ontariohealthathome.ca
IMPORTANT: DO NOT send any personal health information. This email is not for patient feedback or referrals. Please call us directly at the numbers listed above. We aim to respond within 72 hours, however, this email account is not checked on weekends or statutory holidays.
IMPORTANT: DO NOT send any personal health information. This email is not for patient feedback or referrals. Please call us directly at the numbers listed above. We aim to respond within 72 hours, however, this email account is not checked on weekends or statutory holidays.
Visit South West Healthline
South West Area Office Locations
-
London(Corporate Office)
356 Oxford Street West,
London, ON, N6H 1T3
Fax: 519-472-4045 -
Owen Sound
1415 1st Avenue West,
Suite 3009,
Owen Sound, ON, N4K 4K8
Fax: 519-371-5612 -
St. Thomas
1063 Talbot Street,
Unit 70,
St. Thomas, ON, N5P 1G4
Fax: 519-631-2236 -
Stratford
65 Lorne Avenue East
Stratford, ON, N5A 6S4
Fax: 519-273-2847 -
Woodstock
1147 Dundas Street,
Woodstock, ON, N4S 8W3
Fax: 519-539-0065
Compliments and Concerns?
Please share your feedback with your care coordinator. You may also share compliments or concerns in the following ways:
Email: sw.feedback@ontariohealthathome.ca
Phone: 519-473-2222 (1-800-811-5146)
Mail:
Ontario Health atHome
Attn: Patient Relations Department
356 Oxford Street West, London, ON N6H 1T3
Newsroom and Media Relations
Visit our newsroom for more information on news and events.
For all media-related enquiries, please contact media@ontariohealthathome.ca.
For non-media-related enquiries, please visit the Contact Us page to access additional contact information.
Accessibility Documents
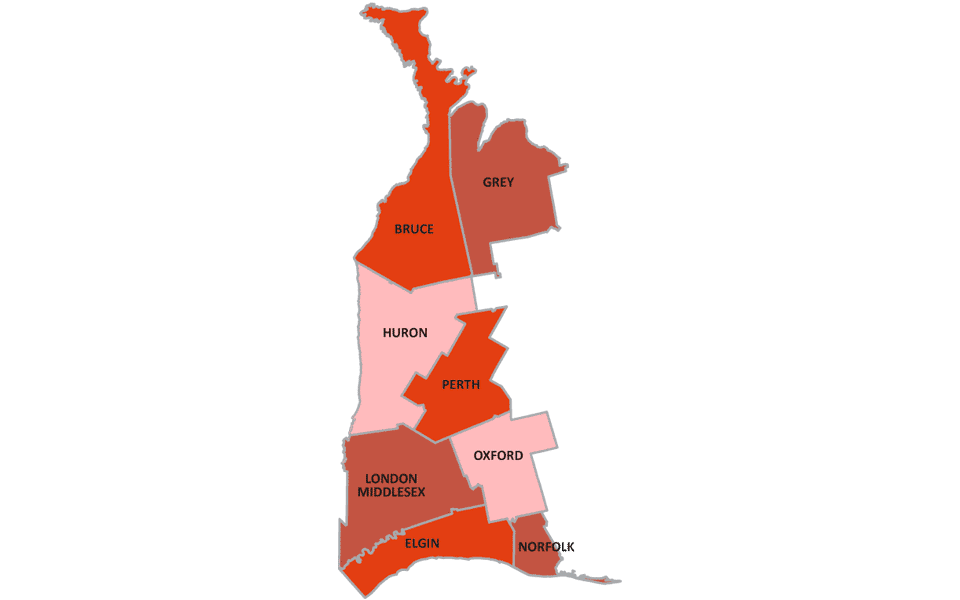
Find a clinic near you in the South West!
(Map updated May 2024)
Forms
| Title | Summary | Region | Last Modified | Category | File Type | File Size | Link | hf:doc_tags | hf:doc_categories | hf:file_type |
|---|---|---|---|---|---|---|---|---|---|---|
| Adult Intravenous Remdesivir Infusion Therapy Order Form – EN | Ministry of Health only provides coverage for a maximum of three doses for an eligible patient. Determining and providing proof of patient eligibility for IV Remdesivir therapy is the Prescriber’s responsibility, namely: The individual does not require hospitalization; AND the individual cannot take Paxlovid (nirmatrelvir and ritonavir), e.g., due to a drug interaction or contraindication;AND the individual has a positive COVID-19 test result (molecular or rapid antigen) and has had symptoms for fewerthan 8 days at the time treatment is initiated (dose 1). | South West | July 3, 2024 | Forms | 469 KB | south-west | forms | |||
| Adult Parenteral Antibiotic Therapy Order Form – EN | Orders are processed between 8 am– 8pm, 7days/week and require a minimum 4-hour turn around window. | South West | July 3, 2024 | Forms | 280 KB | south-west | forms | |||
| Adult Standard Flush Protocol – EN | … | South West | July 3, 2024 | Forms | 314 KB | south-west | forms | |||
| ARCHES – Short-Term Transitional Care Program – EN | Through our Available Retirement Care Home Enhanced Supports (ARCHES) to Care Beds Program, we are able to help you move from the hospital to a retirement residence with enhanced supports where you can make important decisions about your future care and living arrangements. | South West | July 3, 2024 | Forms, Information Sheet | 559 KB | south-west | forms information-sheet | |||
| Diabetes Type 1 Request Treatment Order – EN | Request for Type 1 Diabetes Treatment Order | South West | July 3, 2024 | Forms | 92 KB | south-west | forms | |||
| Enteral Feeding Form – Adult – EN | … | South West | July 3, 2024 | Forms | 121 KB | south-west | forms | |||
| Formulaire de demande pour la divulgation de renseignements personnels | Formulaire de demande pour la divulgation de renseignements personnels. En vertu de la Loi de 2004 sur la protection des renseignements personnels sur la santé Veuillez | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | July 8, 2024 | Forms | 2 MB | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | |||
| Hydration Form – EN | … | South West | July 3, 2024 | Forms | 214 KB | south-west | forms | |||
| IV First Dose and Iron Sucrose Screener – EN | … | South West | July 3, 2024 | Forms | 163 KB | south-west | forms | |||
| MAID Referral Form – EN | South West MAID referral form | South West | July 3, 2024 | Forms | 202 KB | south-west | forms | |||
| MHAN Referral Form – EN | Mental Health and Addictions Nursing Program Referral Form | South West | July 3, 2024 | Forms | 122 KB | south-west | forms | |||
| Negative Pressure Wound Therapy Referral Form | Note: NPWT will continue to be assessed in the community, and settings may be reviewed based on exudate and patient tolerance. Continuation of NPWT is dependent on wound healing goals being met. Maximum treatment time for NPWT is 8 weeks. | South West | July 19, 2024 | Forms | 2 MB | south-west | forms | |||
| Pain Management Order Form – EN | … | South West | July 3, 2024 | Forms | 247 KB | south-west | forms | |||
| Palliative Care – Community Services Assessment Request – EN | Request for palliative services in the community | South West | July 10, 2024 | Forms | 215 KB | south-west | forms | |||
| Physician Notification of Concern or Compliment – EN | … | South West | July 3, 2024 | Forms | 141 KB | south-west | forms | |||
| Referral/Request for Assessment – EN | Referral/Request for Assessment in South West area.This is a PDF Interactive form. You have the option to complete all or parts, electronically. When completed, please print and fax to Ontario Health atHome. | South West | July 3, 2024 | Forms | 508 KB | south-west | forms | |||
| Request for Release of Personal Health Information | Request for Release of Personal Health Information under the Personal Health Information Protection Act, 2004 | Central, Central East, Central West, Champlain, Erie St. Clair, Global, Hamilton Niagara Haldimand Brant, Mississauga Halton, North East, North Simcoe Muskoka, North West, South East, South West, Toronto Central, Waterloo Wellington | July 8, 2024 | Forms | 2 MB | central central-east central-west champlain erie-st-clair global hamilton-niagara-haldimand-brant mississauga-halton north-east north-simcoe-muskoka north-west south-east south-west toronto-central waterloo-wellington | forms | |||
| Symptom Response Kit Prescription Form – EN | … | South West | July 3, 2024 | Forms | 2 MB | south-west | forms | |||
| Wound Consult Request – Virtual – EN | A referral form to request a virtual wound consult with an NSWOC/WCS/ET or Nurse Practitioner from the South West Regional Wound Care Program. | South West | July 3, 2024 | Forms | 292 KB | south-west | forms |